Runner's Knee - Why Rest Alone Doesn't Work
In this blog post and video, I dive into the frustrating cycle of runner's knee and why simply resting might not be the solution you think it is. I explain how the pain is often a symptom of deeper issues related to the kinetic chain, particularly involving the hip and ankle. By understanding the interplay of muscles and how they affect knee alignment, we can break the cycle of pain. I outline a three-stage recovery process: relieve, restore, and elevate, emphasizing the importance of retraining the right muscles. I encourage you to consider whether your knee is truly the culprit or just a victim of other underlying problems.
⏱️ TIMESTAMPS:
0:00 - Understanding Runner's Knee: The Frustrating Pattern
1:08 - Identifying the Cause: Beyond Training Errors
1:31 - Assessing the Knee: The Train on Rails Analogy
2:07 - Analyzing Muscle Imbalance: The VMO vs. IT Band Tug-of-War
3:09 - Investigating Upstream and Downstream Effects
4:33 - Understanding the Biomechanical Puzzle: East Meets West
5:43 - Implementing a Recovery Plan: The 3 Stages
6:37 - Viewing the Body as a System
Identifying the Cause: Beyond Training Errors [1:08]
Runner's knee stems from multiple factors - training errors, direct injury, IT band problems - but one pattern appears consistently in distance runners: kinetic chain dysfunction. This isn't just about your knee. It's about how forces from your hip above and your ankle below converge at your kneecap, creating the perfect storm for pain.
Multiple causes exist: Bad training habits, direct trauma, IT band tightness, structural variations
Kinetic chain dysfunction is common: Weakness or restrictions above and below the knee create compensation patterns
Focus shifts upstream and downstream: The knee is often the victim, not the villain
Understanding this changes everything about how you approach recovery.

The Train on Rails: How Your Kneecap Tracks [1:31]
Picture your kneecap as a train that needs to glide smoothly down a set of rails - the groove on your thigh bone (femur). When everything works properly, that train stays perfectly centered. But when the rails themselves get rotated from hip dysfunction, or when the track gets torqued from ankle problems, the train can't possibly stay on course.
Perfect tracking = pain-free running: Kneecap glides centered in its femoral groove
Rails get rotated: Weak hips cause femoral internal rotation, angling the groove wrong
Track gets torqued: Stiff ankles force knee compensations, twisting the whole system
No amount of train maintenance helps if the rails are crooked: Rest can't fix misaligned forces
This analogy reveals why local knee rest fails - you're not fixing the track itself.
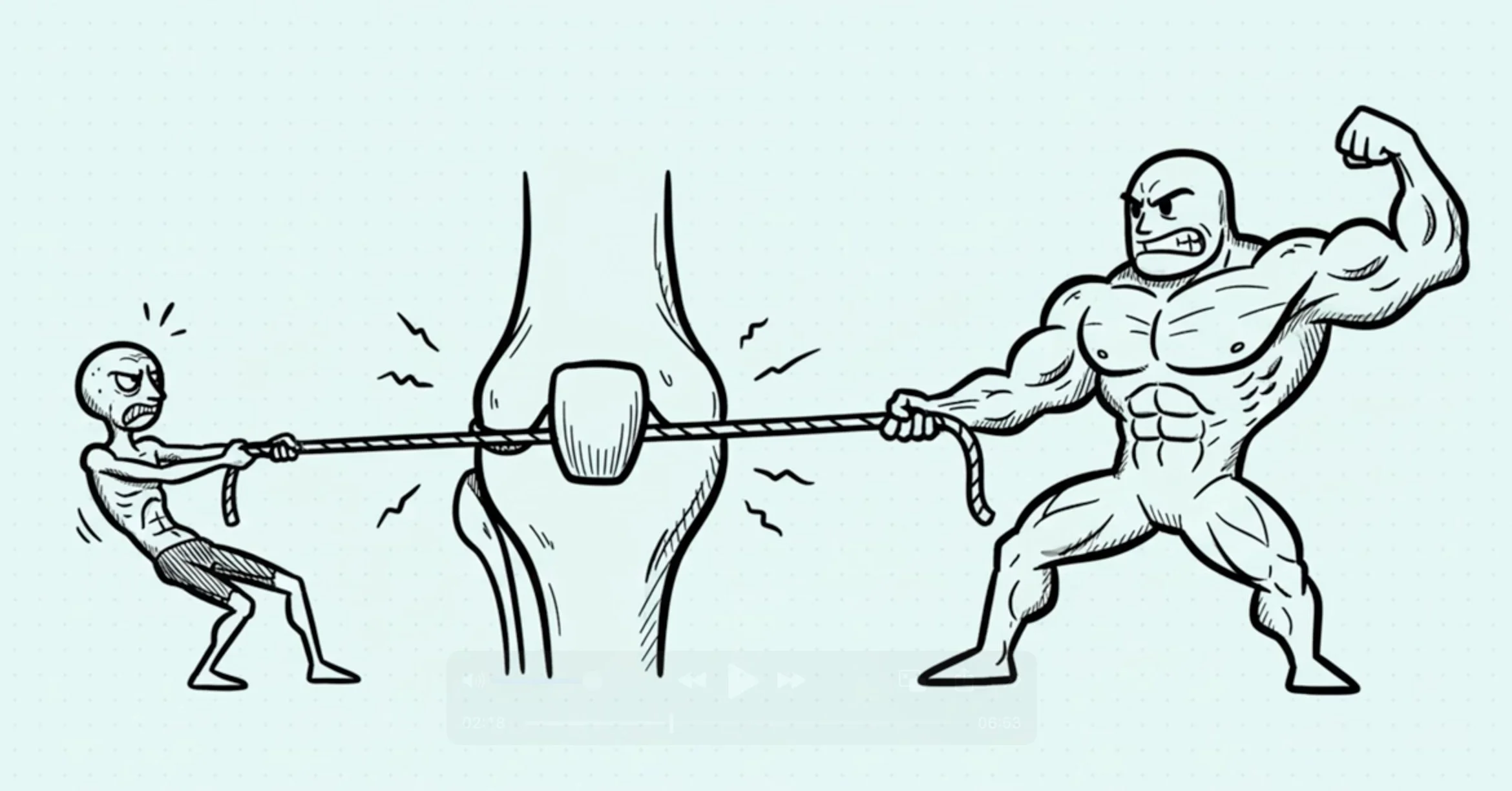
The VMO Tug-of-War: Muscle Imbalance Explained [2:07]
Safety protocols work best when patients feel empowered to ask questions. Here's what you should feel comfortable asking.
Patients should feel empowered to ask about safety protocols
Practitioners should be willing to show the sealed package and explain the safety measures
A good practitioner welcomes these questions. If asking about safety feels uncomfortable, that's a red flag.


Upstream and Downstream: The Kinetic Chain [3:09]
Your knee doesn't exist in isolation. Weak hip muscles - especially the glute medius - allow your pelvis to drop during running, forcing your thigh bone to rotate inward. This rotates the "rails" we discussed earlier. Meanwhile, limited ankle dorsiflexion from tight calves or old sprains forces your body to compensate by turning your foot out or collapsing your knee inward. Your knee is getting attacked from both directions.
Weak hips above: Glute medius weakness → pelvic drop → femoral internal rotation → rotated rails
Stiff ankles below: Limited dorsiflexion → compensatory foot turn-out or knee valgus → abnormal torque
Knee caught in the middle: Absorbing dysfunctional forces it was never designed to handle
Rest can't fix hip weakness or ankle stiffness: The underlying mechanical drivers remain
This is why comprehensive assessment matters - we need to find where your specific kinetic chain is breaking down.
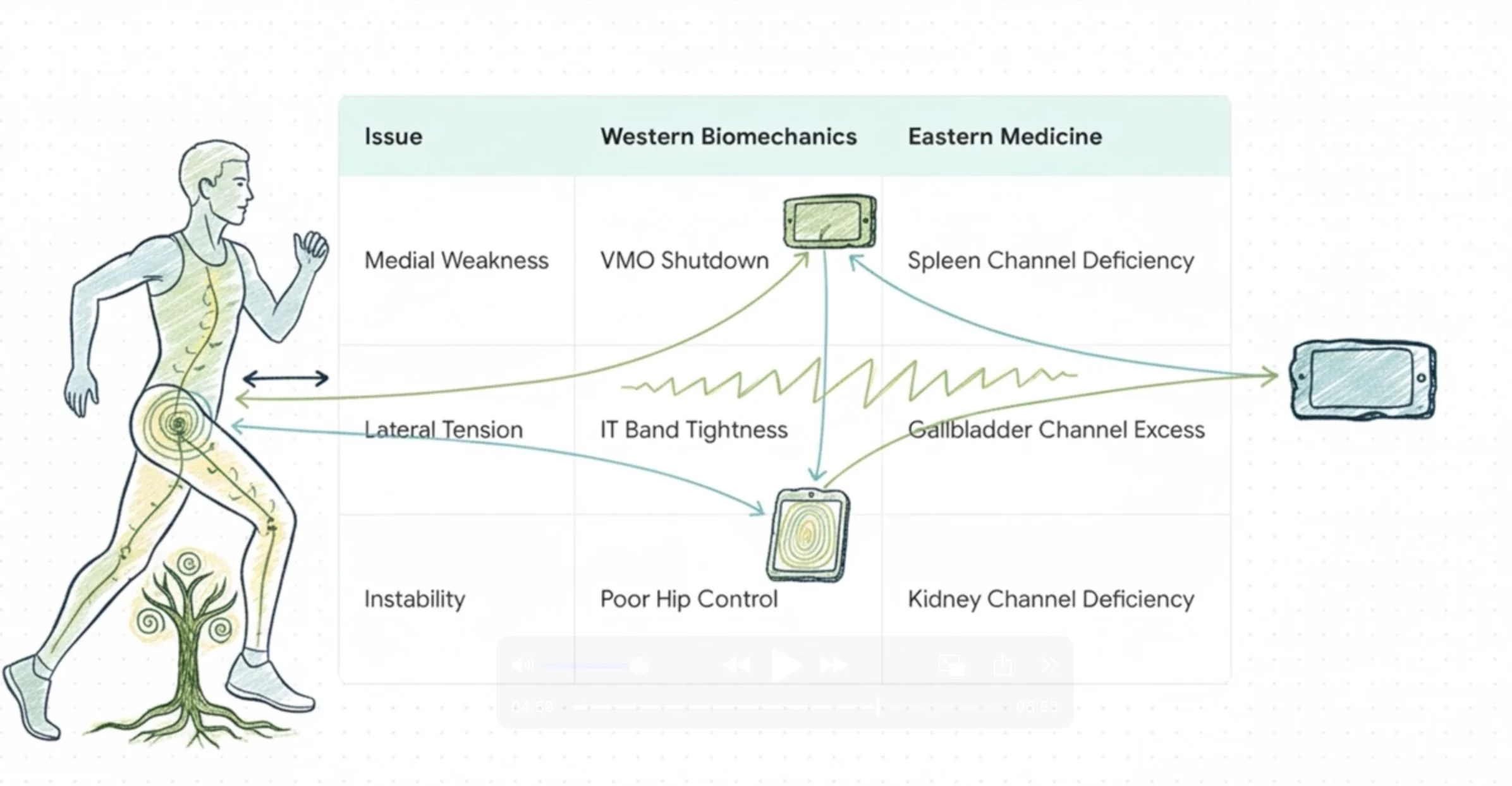
East Meets West: Two Maps, Same Territory [4:33]
Western biomechanics sees VMO weakness and IT band tightness. Eastern medicine sees Spleen channel deficiency (runs through the VMO, governs medial stability) and Gallbladder channel excess (runs through the IT band, creates lateral tension). They're describing the exact same dysfunction through different lenses - and both lead to the precise anatomical locations that need treatment.
VMO motor point = Spleen channel pathway: SP10 area where nerve enters muscle
IT band tension = Gallbladder channel excess: GB31, GB34 points along lateral thigh and knee
Channels aren't mystical: They're anatomical highways connecting motor points, trigger points, fascial pathways
Both systems guide treatment: Motor point retraining + channel balancing = comprehensive recovery
The integration of Western neuroscience and Eastern channel theory creates a treatment approach that addresses both the mechanical dysfunction and the energetic imbalance simultaneously.
Questions about how this kinetic chain pattern might apply to your specific knee pain? Assessment reveals YOUR unique dysfunction pathway - complimentary 15-minute assessments available at Funktion Acupuncture in San Diego.
Runner's Knee: Why Rest Alone Doesn't Work - Acupuncture Treatment in San Diego
If you're a runner struggling with knee pain, you know the maddening cycle. Your knee hurts, so you rest. After a week, it feels better. You lace up your shoes, feeling optimistic, only to have that familiar ache return by mile three or four. You rest again, maybe longer this time, but the outcome is the same. This rest-resume-hurt-repeat pattern is deeply frustrating and can make you question if you'll ever run pain-free again.
The fundamental reason this cycle occurs is that rest addresses the symptom—inflammation in the knee—but not the root cause. Your knee is the messenger, loudly delivering the news of a problem. But the problem itself frequently originates from elsewhere in your body. Rest quiets the messenger, but the moment you resume running, the underlying mechanical problems send the same painful message.
It's important to understand that runner's knee (patellofemoral syndrome) can develop from many different causes: training errors and overuse, direct trauma to the kneecap, structural variations like patella alta (high-riding kneecap), IT band tightness, meniscus issues that mimic knee pain, or the pattern we're focusing on here—the kinetic chain dysfunction pathway.
This article explores ONE common pattern I frequently see in distance runners at my San Diego practice, not THE only cause of runner's knee. This specific pattern—VMO motor point shutdown combined with problems from the hip above and ankle below—explains why rest alone so often fails for many athletes. However, a proper assessment is always required to determine if this is the specific pattern driving YOUR pain, or if other factors are involved.
Understanding this kinetic chain mechanism is an important first step toward breaking the cycle and exploring effective treatment like sports medicine acupuncture for runner's knee in San Diego.
Understanding Runner's Knee - The Vicious Cycle and Its Cause
To understand this pattern of runner's knee, we first need to look at basic knee mechanics. A helpful analogy is to think of your kneecap (patella) as a "train" that should glide smoothly on its "rails" (the trochlear groove of the femur). When everything is balanced, this movement is effortless and pain-free.
This balance is maintained by a constant "tug-of-war" between the muscles on the inside and outside of your thigh. The Vastus Medialis Obliquus (VMO), located on the inner part of your quad, pulls the kneecap medially. The powerful Vastus Lateralis (VL) and the iliotibial (IT) band pull it laterally. A balanced pull keeps the train perfectly centered on the rails.
The VMO, however, is notoriously prone to "shutting off." Research shows that even minor knee inflammation or a past injury can cause its reflex inhibition. This is because the distinct "nerve twigs" that supply the VMO also innervate the medial joint capsule of the knee.
Inflammation in the capsule can directly disrupt the nerve signal through a reflex arc, creating a vicious cycle: pain causes VMO shutdown, which causes worse tracking, which causes more pain. When this happens, the lateral structures win the tug-of-war unopposed, pulling the kneecap off its tracks and causing friction, inflammation, and pain.
In my San Diego practice during marathon season, runner's knee is one of the most common presentations. Almost every runner tells me the same story: rest helps, but running brings it right back. The pattern typically emerges around weeks 8-12 of training, when weekly mileage surpasses the 30-40 mile threshold.
This isn't a coincidence. At lower volumes, the body can compensate for the underlying dysfunction. But as the mileage and repetitive load increase, the body's ability to compensate breaks down, and the knee becomes the painful weak link.
The Kinetic Chain Dysfunction: Three-Part Mechanical Failure
The pain you feel in your knee is often the final outcome of a cascade of mechanical failures happening elsewhere. It's a breakdown in the kinetic chain that unfolds in a cause-and-effect spiral involving local instability at the knee, descending dysfunction from the hip, and ascending dysfunction from the ankle.
1. VMO Motor Point Shutdown: The Local Stabilizer Goes Offline
The VMO's primary job is to provide medial stability. Its fibers attach to the patella at a crucial 50-55 degree angle, perfectly positioned to counteract the powerful lateral pull of the VL and IT band.
The motor point is where the nerve enters the muscle to make it contract. When this motor point shuts down due to reflex inhibition, the VMO goes offline. The lateral structures now win the "tug-of-war" with every single step, pulling the kneecap off track and grinding it against the femur.
2. Descending Dysfunction: How a Weak Hip Rotates Your "Rails"
More often than not, the VMO shutdown is just a symptom of a larger problem cascading from above. Pelvic instability or weakness in the hip abductor muscles, like the gluteus medius, forces the femur to rotate internally and drift inward. This is called descending dysfunction because the problem starts higher up the chain.
This mechanical failure means the "rails" themselves are now angled incorrectly. Even if the VMO were firing perfectly, it becomes impossible for the kneecap to track properly because its track is misaligned. The VMO is being asked to do an impossible job, and it inevitably fatigues and shuts down.
3. Ascending Dysfunction: When Ankle Limitations Torque the Knee
At the same time, problems from below can transmit abnormal force up to the knee. Our gait depends on a smooth transition through the "ankle rocker," which requires adequate ankle dorsiflexion (the ability of the shin to move over the foot).
If this movement is restricted, the body is forced to compensate. Common compensations include turning the foot out or allowing the knee to collapse inward (knee valgus). These movements transmit abnormal torque and stress directly up to the knee, further overwhelming the already-inhibited VMO and creating an environment where it simply cannot win.
Eastern Medicine Perspective: Channel Imbalance and Runner's Knee
This kinetic chain dysfunction can be understood through two complementary lenses: modern biomechanics and traditional Eastern medicine. Western biomechanics identifies VMO weakness and IT band tightness. Eastern medicine maps this to Spleen channel deficiency (medial weakness) and Gallbladder channel excess (lateral tightness).
Same dysfunction, two complementary maps leading to the exact anatomical locations that need treatment with runner's knee acupuncture.
VMO Shutdown & Spleen Deficiency: The Spleen channel in Eastern medicine governs muscle activation and runs directly through the VMO area, with a key point (SP10) located right at its motor point. A deficient Spleen channel means the motor point lacks the energetic support to fire properly and sustain contraction under load.
VL/IT Band Dominance & Gallbladder Excess: The Gallbladder channel runs down the lateral leg, directly along the path of the IT band and Vastus Lateralis. "Excess" in this channel manifests as the hypertonicity, trigger points, and tightness that biomechanically overpower the medial structures.
Hip Abductor Weakness & Gallbladder Channel Imbalance: Western biomechanics sees a weak gluteus medius leading to pelvic drop. The Gallbladder channel governs this lateral stability. Its dysfunction can manifest as both excess tension down the IT band and deficiency or weakness at the hip, explaining why the entire lateral chain fails as a unit.
Pelvic Instability & Kidney Deficiency: The Kidney channel is considered the foundation of the body's deep, structural strength and stability. A deficiency here often correlates with the underlying pelvic instability and weak deep hip rotators that drive the descending dysfunction from the hip.
These channels are not mystical energy lines. They can be understood as "anatomical highways" that connect motor points, trigger points, and fascial pathways. This isn't woo-woo energy work—it's applied neuroscience guided by channel theory. The ancient maps lead us to the exact anatomical locations where modern science shows the dysfunction is occurring.
Sports Medicine Acupuncture Treatment for Runner's Knee in San Diego
Resolving this pattern requires a systematic approach that goes beyond just treating the knee. Before any treatment begins at my San Diego practice, I perform comprehensive detective work to map out your specific pattern of dysfunction.
The Detective Work: A Comprehensive Assessment
Manual Muscle Testing: We test the activation of your VMO and the strength of your gluteus medius. Athletes are often shocked when they try to contract their quad and can feel that their VMO isn't firing at all.
Movement Assessment: A gait analysis reveals compensation patterns like a "cross-over" stride. A single-leg squat immediately shows whether the VMO can control the lateral pull—if your knee collapses inward, we know motor control has been compromised.
Trigger Point Mapping: I palpate the muscles of your thigh, like the VL, TFL, and IT band. I can often reproduce their exact knee pain by pressing on a trigger point in the lateral thigh. That's the moment they understand why foam rolling alone didn't work.
Channel Palpation: I assess the Spleen, Gallbladder, and Kidney channels to confirm the pattern of medial deficiency and lateral excess.
Functional Tests: We check for limitations in key movements like the ankle rocker (dorsiflexion) to identify any ascending dysfunction.
The Treatment Plan: Restoring the Kinetic Chain
Based on the assessment, the treatment plan is designed to systematically restore function from the ground up and the hip down. This integrated sports medicine acupuncture approach includes:
Motor Point Retraining: This is the central part of the treatment. We use precise electrical stimulation on the VMO motor point and glute medius motor points to "wake up" the nerve-muscle connection and retrain the brain to activate these inhibited muscles correctly. This isn't vague energy work—it's precise neuromuscular therapy at the exact location where the nerve enters the muscle.
Trigger Point Release: Needling trigger points in the VL, IT band, and TFL releases the chronic tension that creates the unopposed lateral pull on the kneecap. These trigger points often refer pain directly to the knee, perpetuating the problem even when the VMO starts to activate.
Channel Point Selection: We select key acupuncture points to support the system. SP9 and SP10 tonify medial support along the Spleen channel. GB31 and GB34 release lateral excess along the Gallbladder channel. KD3 supports the body's foundational stability through the Kidney channel. Local knee points like ST35 and ST36 address inflammation and restore proper function.
The Recovery Journey: Stages of Care
Progression varies for everyone based on the chronicity of the injury, training load, and compliance. There are no fixed session counts. Instead, we progress through stages of care as your body adapts.
Stage 1 (Relieve): The initial focus is on calming the irritated knee, releasing the most active trigger points, and beginning VMO activation. In this stage, athletes notice less pain with daily activities like walking or using stairs. Early in treatment, you'll feel the acute inflammation settling.
Stage 2 (Restore): This is the core of the work. We focus on intensive motor retraining of the VMO and glutes, addressing hip and ankle mechanics, and balancing the channels.
As treatment progresses over weeks into Stage 2, something different happens: you start to feel your VMO fire, maybe for the first time in months. Your single-leg stability improves. You can typically resume light running. This stage cannot be rushed—the nervous system needs time to adopt new patterns. Motor retraining takes time and varies based on how long you've had the compensation pattern.
Stage 3 (Elevate): Once function is restored, the focus shifts to maintenance, supporting increased training loads, and catching early imbalances before they become painful. For many athletes in heavy training, this may involve monthly "tune-ups" at my Kearny Mesa clinic.
Prevention and Training Integration for Runners
Understanding this kinetic chain pattern empowers you to be proactive about prevention and to train smarter, whether you're training in San Diego's hills or preparing for a destination marathon.
The Prevention Window: The key time to intervene is not when you're in acute pain, but during weeks 6-8 of a training build-up. This is when subtle signs of compensation often appear—vague inner knee awareness around mile 4-6 or your VMO feeling "quiet" during long runs.
Early Warning Signs: I use these concepts in my own marathon training. When I notice my VMO feeling "quiet" during long runs—like it's not engaging fully—that's my signal to get in for a tune-up before it becomes actual pain. Other signs include subtle lateral tightness after a run or slight knee wobble during single-leg balance.
Training Modifications During Treatment: Trying to maintain full running volume will slow your progression through Stage 2. It's often best to incorporate cross-training like swimming or cycling. Weekend appointments are perfect for runner's knee—I can assess and treat you right after your long run when tissues are most reactive and the compensation pattern is fully expressed.
Long-Term Maintenance: To stay healthy, consistently incorporate VMO activation exercises, hip abductor (glute medius) strengthening, and ankle mobility work into your routine. Addressing tight calves and hip flexors before they create compensation patterns is key.
Is This Your Pattern? Why Assessment Matters
We've explored the kinetic chain dysfunction pathway in detail—VMO motor point shutdown combined with descending dysfunction from the hip and ascending dysfunction from the ankle. This is one very common pattern I see in runners, especially during marathon training buildups. But it's important to understand that this is one pathway to runner's knee, not the only pathway.
The rest-resume-hurt cycle strongly suggests kinetic chain dysfunction because rest can't fix a weak hip or a tight ankle. However, your knee pain could stem from different causes:
Pure Training Errors: You ramped up mileage too quickly without underlying mechanical issues. In this case, proper training progression and load management may resolve the issue without extensive kinetic chain work.
Structural Variations: Some runners have patella alta (high-riding kneecap) or trochlear dysplasia (shallow femoral groove). These structural factors change the treatment approach.
Isolated IT Band Tightness: Your IT band could be the primary driver without the full kinetic chain pattern. This responds to targeted IT band work rather than comprehensive hip and ankle correction.
Meniscus Involvement: Sometimes what feels like runner's knee is actually meniscus irritation or a small tear creating similar anterior knee pain.
The timeline and outcome of your recovery will be influenced by several factors unique to you:
Chronicity: An acute issue (less than 3 months) will often resolve faster than a chronic pattern that has been present for years. If you've had runner's knee for 3+ years with complete VMO shutdown, expect motor retraining to take longer than someone who caught it after 3 weeks.
Training Load: Your progression will be different if you are taking full rest versus cross-training versus trying to run through the injury. More load during treatment typically means slower Stage 2 progression.
Compliance: The "homework" matters. Consistently doing your corrective exercises—VMO activation work, glute strengthening, ankle mobility—between sessions significantly speeds up motor retraining.
Upstream/Downstream Complexity: If we need to address both hip dysfunction AND ankle limitations, that's more complex than isolated VMO weakness. Some athletes have the full kinetic chain pattern, others have primarily one contributing factor.
This is why proper assessment is everything. Only a thorough evaluation can determine which pattern is driving YOUR specific knee pain and what treatment approach will be most effective for your unique situation.
Conclusion: Breaking the Cycle with Runner's Knee Acupuncture in San Diego
To break the cycle of runner's knee, it's essential to look beyond the site of pain. The kinetic chain pattern we've explored involves VMO motor point shutdown at the knee, descending dysfunction from the hip, and ascending dysfunction from the ankle.
Rest fails for this pattern because it only addresses the resulting inflammation. It cannot correct the mechanical problems above and below the knee that keep pulling your kneecap off track.
An integrated East-West model provides a complete map of this dysfunction. Sports medicine acupuncture for runner's knee addresses this systematically—retraining motor points with electrical stimulation, releasing trigger points that refer pain to the knee, and balancing the Spleen and Gallbladder channels to restore medial-lateral equilibrium.
Everyone's body and injury history is unique, which means each person's pattern and recovery timeline will differ. Timeline depends on chronicity, training load during treatment, compliance with exercises, and the complexity of your specific kinetic chain dysfunction. This makes an individualized assessment the most important first step toward a lasting solution.
If you're a runner in San Diego stuck in the rest-resume-hurt cycle, a proper assessment is the first step to understanding what's driving your pain. I offer complimentary 15-minute assessments at Funktion Acupuncture where we can test your VMO activation, hip strength, ankle mobility, and identify the trigger point patterns and channel imbalances unique to you. We'll determine if the kinetic chain pattern is your issue or if other factors are involved. Weekend appointments are available to assess you right after your long runs when the dysfunction pattern is most evident.
This content was created with AI assistance (Claude AI & Google NotebookLM) and inspired by comprehensive research on runner's knee kinetic chain dysfunction, including work from Functional Anatomic Palpation Systems on VMO mechanics, descending lesion pathways, gait biomechanics, and fascial chain integration. All clinical insights and Eastern medicine perspectives are from Michael Cohen, LAc, practicing sports medicine acupuncture in San Diego at Funktion Acupuncture.