Acupuncture for Plantar Fasciitis in San Diego: Why It's Probably Nerve Entrapment
In this blog post and video, I dive into the frustrating issue of stubborn heel pain, often misdiagnosed as plantar fasciitis, and explore how it might actually be a symptom of a deeper problem. I share insights on how various factors, like a stuck midfoot, stiff big toe, or weak glutes, can contribute to this pain, emphasizing that the heel may just be the last domino to fall in a complex chain of issues. I encourage you to consider what your heel pain is trying to tell you rather than just trying to silence it. A professional assessment can be a game-changer in identifying your unique combination of factors. Let's shift our focus from merely treating the symptom to understanding the underlying causes.
⏱️ TIMESTAMPS:
0:00 - Introduction: It's Probably Not Plantar Fasciitis
1:04 - The Two Pain Patterns: Nerve vs. Fascia
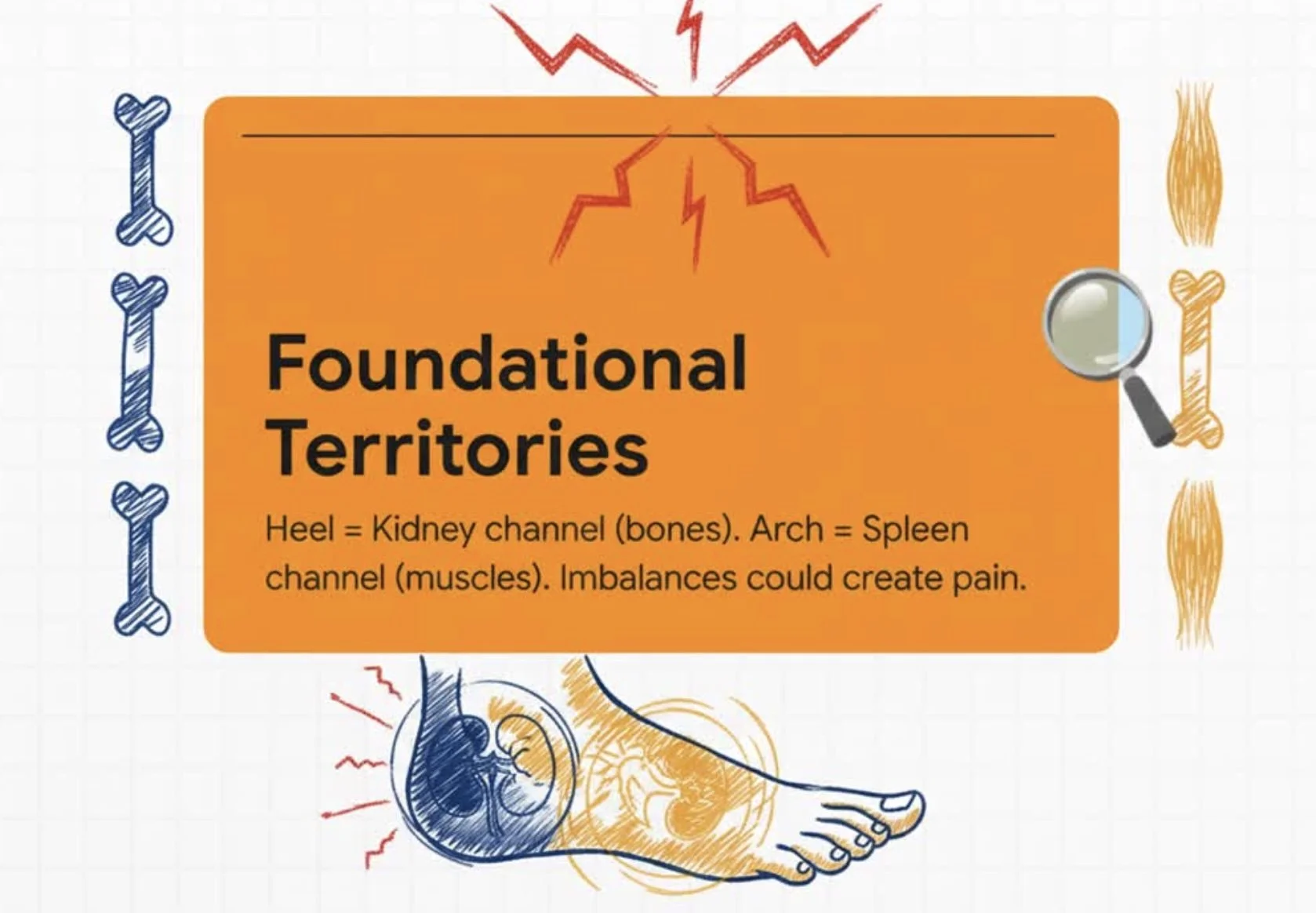
2:09 - Eastern Medicine Foundation: Kidney-Spleen Territory
2:38 - Pathway 1: Navicular Fixation (Midfoot Keystone Stuck)
3:31 - Pathway 2: Cuboid Dysfunction & Gait Rockers
4:15 - Pathway 3: Great Toe Limitation & Baxter's Nerve
4:47 - Pathway 4: Ankle Dorsiflexion Blockage (Old Ankle Sprains)
5:17 - Pathway 5: Tibialis Posterior Weakness (Arch Captain Failure)
5:56 - Pathway 6: Bottom-Up Fascial Chain (Weak Glutes)
7:03 - Why Self-Diagnosis Fails: Multiple Pathways Combining
8:01 - Conclusion: Your Heel Pain Is Information
Identifying Pain Patterns [1:04]
Two distinct pain patterns can reveal whether you're dealing with fascial inflammation or nerve entrapment—and this distinction completely changes the treatment approach.
Morning pain pattern: Severe first thing in the morning but eases with movement—suggests fascial stiffness (true plantar fasciitis)
Activity pain pattern: Increases the longer you're on your feet, doesn't improve with warming up—suggests nerve compression (medial calcaneal or Baxter's nerve)
Why this matters: If you're stretching and icing fascial tissue when the real problem is nerve entrapment, you're treating the wrong structure entirely
Most runners assume all heel pain is plantar fasciitis. But the pain pattern tells a different story.
Exploring Underlying Causes [2:09]
Your heel pain is rarely just about your heel—it's usually the final symptom of dysfunction happening upstream in the kinetic chain.
Stuck midfoot: Navicular bone (arch keystone) loses mobility from old sprains or chronic collapse—creates rigid arch that can't absorb shock
Locked cuboid: External rotation restriction blocks normal pronation—forces compensatory heel strike angles
Eastern medicine view: Navicular sits on Spleen channel (arch support), cuboid on Gallbladder channel (lateral column)—restrictions indicate channel stagnation
Bottom-up cascade: Small midfoot joint fixations create massive heel loading changes with every step
The midfoot controls heel mechanics. When it's restricted, your heel pays the price.
Understanding Biomechanics [3:31]
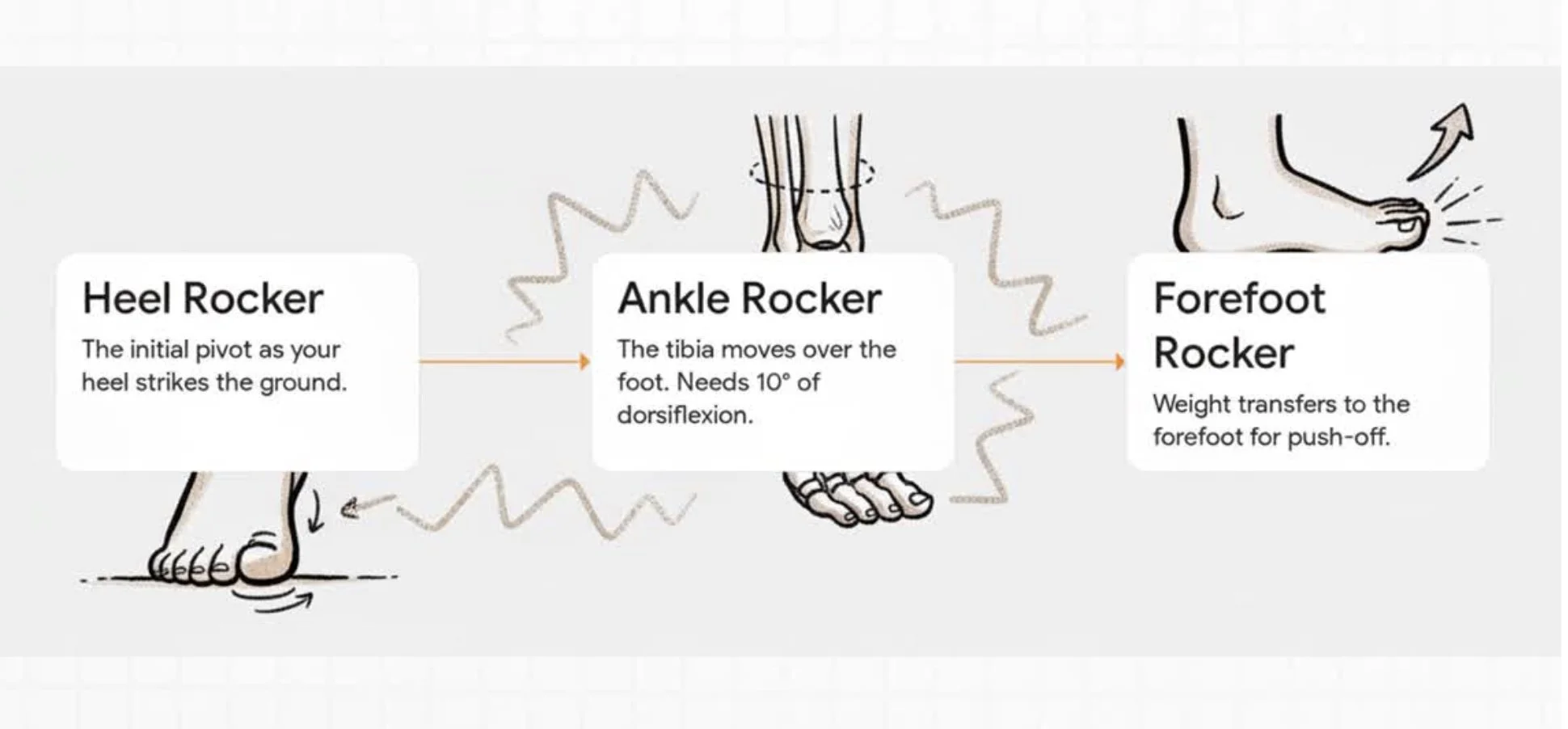
Healthy walking and running require three sequential "rockers"—smooth pivots that transfer body weight from heel strike to toe-off. When any rocker fails, heel loading gets disrupted.
Heel rocker: Initial contact—body weight rocks over the heel from impact to foot flat
Ankle rocker: Major pivot requiring 10° dorsiflexion—tight calves limit this, forcing foot to turn outward and creating abnormal heel angles
Forefoot-toe rocker: Weight transfers to forefoot, great toe extends, you push off—if this fails, heel stays loaded longer trying to compensate
Real example: Runner switches to zero-drop shoes → calves tighten → ankle rocker fails → foot compensates by everting → heel gets loaded at wrong angles → nerve compression develops
One training change can trigger a cascade. Understanding the rockers shows you where the breakdown occurs.
Evaluating Muscle Strength [5:17]
The tibialis posterior—your "arch captain"—is the primary dynamic supporter of your medial arch. When it weakens, your plantar fascia has to do a job it was never designed for.
TP function: Controls arch mechanics during gait, prevents excessive collapse, works with Spleen channel pathway
What happens when it's weak: Plantar fascia becomes the arch supporter instead—massive overload at heel attachment where fascia originates
Eastern medicine correlation: Weak TP IS Spleen deficiency manifesting—same problem, two languages describing it
Assessment signs: Flat feet, chronic overpronation, arch fatigue during runs, medial ankle tenderness
This is one of the clearest East-West correlations in heel pain. TP weakness forces fascial compensation.
Comprehensive Assessment [7:03]
Why does heel pain resist standard treatment? Because it's rarely just one thing—most runners have multiple pathways combining to create that single heel symptom.
Complex example: Bunion limiting great toe → prolonged heel loading + Cyclist with tight calves → failed ankle rocker + Desk job creating weak glutes → posterior chain tension = Four pathways funneling to one heel pain
What assessment reveals: Nerve vs. fascia testing, midfoot bone mobility, arch captain strength, glute activation, gait rocker analysis
Individual solutions: Mobilizing stuck joints ≠ strengthening weak muscles ≠ releasing nerve compression—each pathway needs targeted treatment
Channel integration: Assessment identifies which channels need tonification (Spleen/Kidney deficiency) vs. release (Bladder/Gallbladder excess)
Your heel pain is information. Professional assessment helps decode which specific combination of upstream issues is sending that message.
Curious about YOUR specific pattern? Proper assessment can identify which combination of pathways—navicular restriction, cuboid dysfunction, rocker failure, TP weakness, nerve compression—is creating your heel pain. I offer complimentary 15-minute assessments in San Diego where we test joint mobility, muscle strength, gait rockers, and nerve involvement. Book your assessment
Acupuncture for Plantar Fasciitis in San Diego: Why It's Probably Nerve Entrapment
For many runners dealing with plantar fasciitis, the pattern is frustratingly familiar. That first step out of bed delivers a sharp, stabbing pain in your heel. You hobble for a few minutes, and it eases into a dull ache. "Okay," you think, "it just needs to warm up." But then you go for your run. By mile three, the throb returns, and by mile five, it's sharp again.
You've tried everything. Stretching your calves religiously. Rolling a frozen water bottle under your foot until you're numb. Expensive orthotics that promised arch support. Weeks of rest. Yet the pain always comes back. This frustrating cycle is what leads many runners to seek alternative solutions, including acupuncture for plantar fasciitis, hoping to finally find an answer that sticks.
Here's the reframe I offer in my San Diego practice: Your heel pain might not be the problem itself. It could be the messenger. Think of it like a fire alarm—its job isn't to be the problem, it's to alert you that there's a fire somewhere else. A lot of heel pain diagnosed as plantar fasciitis could actually be nerve entrapment—specifically compression of the medial calcaneal nerve or Baxter's nerve—not inflammation of the plantar fascia itself. This distinction changes everything about how we approach treatment.
In this article, we'll explore several "bottom-up" biomechanical pathways that create heel pain as a downstream symptom. We'll look at how restrictions in your midfoot, failures in your gait mechanics, and even weakness in your hips can manifest as that sharp pain in your heel. This perspective matters because standard plantar fasciitis treatments often fail when they assume all heel pain is fascial inflammation, while the root cause might be a compressed nerve driven by upstream dysfunction that's been completely overlooked.
Understanding Plantar Fasciitis: Nerve Entrapment vs. Fascial Inflammation
First, let's figure out what kind of pain you're actually dealing with—because this distinction tells us everything about treatment.
In my practice, I notice plantar fasciitis pain from fascial inflammation and pain from nerve entrapment often present with two distinct patterns:
Pattern 1: Could Be Fascial Inflammation Pain is WORST first thing in the morning when the fascia is stiff and cold. It typically IMPROVES with initial activity as the tissue warms up and becomes more pliable. This is the classic textbook presentation.
Pattern 2: Could Be Nerve Entrapment Pain WORSENS with activity, like running, as nerve irritation increases with loading. This pain doesn't improve throughout the day—it may actually get progressively worse the longer you're on your feet.
Here's what's happening anatomically. The tarsal tunnel is a narrow space on the inside of your ankle. Through this tunnel pass several key structures, including the Tibial Nerve. This nerve gives off branches that provide sensation to your heel—most notably the medial calcaneal nerve and Baxter's nerve. When the space in this tunnel becomes crowded due to swelling, tight muscles, or altered biomechanics, these nerves get compressed.
This distinction is everything for acupuncture treatment of plantar fasciitis. If you're stretching and rolling fascial tissue when the real problem is a compressed nerve, you're treating the wrong structure entirely. You can't stretch or roll a nerve into health—you must find and address the source of compression.
From an Eastern Medicine perspective, the heel is Kidney channel territory. This channel governs our deep constitutional reserves, structural foundation, and bones. Persistent heel pain often points to a deeper issue in the body's foundational mechanics and capacity.
Bottom-Up Pathway 1: Midfoot Restrictions Create Heel Compensation
One pattern I frequently see with plantar fasciitis is that the problem isn't in the heel at all. It's in the small, complex joints of your midfoot. When the midfoot can't move properly, the heel is forced to compensate, leading to overload.
The Navicular: Your Arch's Keystone
The navicular bone is the "keystone" of your medial arch. It needs to be mobile to allow your foot to pronate (flatten) naturally to absorb shock. When the navicular gets stuck—often from old ankle sprains or chronic arch collapse—it blocks this essential motion. Your foot becomes a rigid lever instead of an adaptive spring, forcing the heel to take on excessive impact.
In acupuncture theory, the navicular lies directly on the Spleen channel pathway. A fixation here is Spleen channel stagnation—disrupting the channel's role in supporting the arch and leading to collapse of the foot's energetic and physical structure. Not everyone has navicular restrictions, but when they're present, they're a major driver of downstream heel pain.
The Cuboid: The Lateral Column Lock
On the outside of your foot, the cuboid bone is critical for lateral column function. If the cuboid gets stuck in internal rotation—another common result of ankle sprains—it locks the outside of your foot. This blocks normal pronation and forces you to alter your gait angle, pushing off the inside of your foot and overloading the heel from a different direction.
This lateral aspect is governed by the Gallbladder channel, and this dysfunction represents Gallbladder channel stagnation. It's a clear example that, just like runner's knee often stems from hip and foot dysfunction, heel pain is rarely just a heel problem.
Connecting Midfoot to Heel
In short, rigidity in either the medial (navicular) or lateral (cuboid) column removes the foot's natural shock absorption. That force has to go somewhere, and it's often transferred directly into the heel—creating tissue strain and potential nerve compression in the tarsal tunnel. This is one reason why acupuncture for plantar fasciitis addresses these upstream midfoot restrictions, not just the symptomatic heel.
How Gait Dysfunction Contributes to Plantar Fasciitis
Efficient walking and running depend on a smooth, three-part sequence called gait rockers. When any part of this sequence fails, the heel is often forced to compensate—and this is where plantar fasciitis symptoms develop.
The Three Rockers of Gait
Picture your stride as three sequential pivots:
1. Heel Rocker: Your heel hits the ground first and acts as a pivot, allowing your body's momentum to roll forward over the foot.
2. Ankle Rocker: As your shin moves forward over your fixed foot, your ankle must bend. This requires at least 10 degrees of dorsiflexion (shin moving toward the foot).
3. Forefoot-Toe Rocker: Finally, your heel lifts, and you push off from the ball of your foot and, crucially, your great toe.
How Rocker Failure Creates Heel Overload
Many runners I see in San Diego have chronically tight calves, which severely limits the ankle rocker. When you can't get that necessary 10 degrees of dorsiflexion, your body finds a workaround—but it comes at a cost to the heel. Your foot might turn outward to fake the dorsiflexion you need, creating abnormal angles of force through the heel with every step.
Similarly, if your great toe is stiff and can't extend properly, it disrupts the forefoot-toe rocker. This causes your heel to stay on the ground longer during each step, dramatically increasing its load time and cumulative stress. Which rocker fails varies by individual—some runners have primarily ankle rocker issues, others struggle with forefoot-toe mechanics—but the result is often the same: heel overload.
From an Eastern Medicine perspective, the posterior chain (including the calves) is Bladder channel territory. The great toe is Liver channel territory. Dysfunction in either area disrupts the smooth flow of Qi and movement, creating downstream compensation at the heel.
Video Explainer
I explain the three gait rockers and how their failure creates heel compensation in detail in this video: [INSERT YOUTUBE VIDEO HERE]
The Great Toe and Baxter's Nerve Compression Pattern
The Role of the Great Toe in Propulsion
The great toe is far more important for powerful, efficient movement than most people realize. For a strong push-off, it needs to extend at least 65 degrees. When that motion is limited by issues like bunions, arthritis (hallux limitus), or turf toe, a specific and problematic pattern emerges that directly contributes to plantar fasciitis.
The Double Problem
A dysfunctional great toe creates a two-part problem that leads to heel pain:
1. Prolonged Heel Loading: Without a powerful push-off from the great toe, your heel is forced to stay on the ground longer to try and generate momentum. This extended loading phase significantly increases strain on heel structures—both the plantar fascia attachment and the nerves in the tarsal tunnel.
2. Direct Nerve Compression: The altered mechanics from poor push-off cause a deep foot muscle called the quadratus plantae to tighten and overwork. Baxter's nerve runs right next to this muscle. As the muscle becomes chronically tight, it directly compresses the nerve, causing sharp, burning, or aching pain on the inside of the heel.
This is why acupuncture for plantar fasciitis often includes treatment of the great toe complex and quadratus plantae trigger points—we're addressing both the prolonged loading mechanism AND the nerve compression pathway.
East-West Coordination
This pattern highlights how different systems must coordinate. The great toe itself is Liver channel territory, while the first metatarsal bone it connects to is part of the Spleen channel pathway. For powerful and pain-free propulsion, both channels must function and coordinate properly. Not everyone with plantar fasciitis has great toe limitation, but when it's present, it's often a major contributor.
When Your "Arch Captain" (Tibialis Posterior) is Weak
While many people focus on the plantar fascia for arch support, the primary dynamic supporter of your medial arch is actually a muscle called the tibialis posterior (TP). I often refer to it as the "arch captain."
Tibialis Posterior: The Primary Arch Supporter
Picture the TP running down the inside of your shin, behind your ankle bone, connecting to the navicular and other bones in your midfoot. Its job is to control the rate of pronation and actively hold up your arch during every step.
When the TP is weak or inhibited, the arch collapses excessively. When this happens, the plantar fascia is forced to take on a job it wasn't designed for—acting as the primary support structure. This leads to massive overload and strain right where the fascia attaches to the heel bone.
The Clearest East-West Correlation
This is one of the clearest East-West correlations I see in my practice: the Tibialis Posterior muscle runs directly on the Spleen channel pathway. Weakness in this muscle literally IS Spleen deficiency. It's the same problem described in two different but complementary languages.
One sees a biomechanical failure of a specific muscle; the other sees an energetic deficiency in the channel that governs that muscle's function. When treating plantar fasciitis with acupuncture, addressing both the TP motor point (to restore muscle function) and the Spleen channel (to tonify the underlying deficiency) creates comprehensive treatment that works on multiple levels simultaneously.
The Posterior Fascial Chain—A Hip Problem Creating a Heel Symptom
Your body isn't a collection of separate parts—it's an interconnected system. The posterior fascial chain is a perfect example, and understanding it is crucial for effective acupuncture treatment of plantar fasciitis.
One Continuous System
Imagine a single, continuous band of connective tissue running from the bottom of your foot (the plantar fascia), up your Achilles tendon, through your calves (gastroc-soleus), up your hamstrings, and connecting all the way into your glutes. This entire system is linked. Tension or weakness in one area inevitably affects the others.
Weak Glutes, Tight Calves, Painful Heel
Here's a pattern I frequently see in runners who also have desk jobs. Sitting weakens the glutes. When the glutes aren't strong enough to provide powerful hip extension for propulsion, the calves are forced to overwork to pick up the slack.
This chronic calf tension travels down the fascial chain, creating a constant pull on the Achilles and plantar fascia at the heel. Furthermore, this gastroc-soleus tightness can also compress the medial calcaneal nerve proximally, causing referred pain into the heel—that nerve entrapment pattern we discussed earlier.
Everyone's fascial chain responds differently to training stress and compensatory patterns. Some runners develop tightness quickly, others maintain more flexibility despite weakness. The key is identifying your specific pattern.
In Eastern medicine, this entire line is the Bladder channel. When this channel is in a state of excess tension, it creates deficiency in the Kidney channel territory (the heel). This is a classic example of how posterior fascial chain issues often appear together—Achilles tendinitis and plantar fasciitis share the same bottom-up causes.
Sports Medicine Acupuncture for Plantar Fasciitis in San Diego
My process for treating plantar fasciitis with acupuncture begins not with needles, but with detective work. Because heel pain can stem from so many different upstream causes, the first step is always a thorough assessment to uncover which combination of pathways is driving your unique pain.
Assessment First: Finding Your Unique Pattern
This assessment might include:
Nerve compression tests to help differentiate nerve involvement from purely fascial pain.
Joint mobility testing to check for restrictions in the navicular, cuboid, and talus bones.
Muscle strength testing of key stabilizers like the tibialis posterior and glutes—weakness here often drives compensatory heel loading.
Gait analysis to identify which of the three rockers may be failing and where compensations show up in your stride.
Channel palpation to feel for tenderness or stagnation at key acupuncture points like SP6 and KI3, which often correlate with biomechanical dysfunction.
In my San Diego practice, I almost always find that the key Spleen and Kidney channel points near the ankle are exquisitely tender—often 8-9/10 pressure pain—on runners with chronic plantar fasciitis. This tenderness correlates directly with navicular restriction and arch collapse patterns.
Integrated and Precise Treatment
Once we've identified the primary drivers, acupuncture treatment for plantar fasciitis is tailored specifically to your pattern. This involves a combination of techniques targeting different tissues with high precision:
Motor Points: Acupuncture needles stimulate the nerve that supplies a weak or inhibited muscle—like needling the tibialis posterior motor point to restore its proper arch support function, or targeting glute motor points to address posterior chain weakness.
Trigger Points: Needling releases tight, compensating muscles like the gastroc-soleus in the calf or the quadratus plantae deep in the arch that may be compressing nerves. In my San Diego practice, I can often reproduce a runner's exact heel pain by pressing these trigger points—this immediately shows them the nerve is involved, not just the fascia.
Channel Points: We use classical acupuncture points to address underlying energetic patterns on the Spleen, Kidney, Bladder, Liver, and Gallbladder channels to support the body's foundational health and restore proper Qi flow.
This integrated approach of using motor point and trigger point needling for heel pain allows us to address both the biomechanical faults and the underlying energetic imbalances contributing to them. It's this combination that makes acupuncture for plantar fasciitis effective where other treatments have failed.
A Clinical Observation
Weekend appointments work particularly well for runners with plantar fasciitis—I can treat you right after your long run when your compensatory patterns are most active and obvious in gait analysis, and when tissues are most reactive to treatment. Early in treatment, you'll likely notice pain reduction and improved morning stiffness. As treatment progresses over weeks, we address the root causes—restoring midfoot mobility, retraining motor patterns, releasing fascial chain tension. Treatment timeline varies based on how long you've had the condition, your training load during treatment, and how your individual body responds to motor point retraining.
Conclusion: Your Heel Pain is Information
If you've been battling heel pain for months with no lasting relief, here's the core message: most chronic heel pain diagnosed as plantar fasciitis could be nerve entrapment with complex, bottom-up causes. It's rarely just one thing.
A common combination I see is a bunion limiting the great toe, tight calves from cycling, and weak glutes from a desk job—all funneling down to create one symptom in your heel. This is why generic, single-cause treatments so often fail. Different bodies develop different combinations of these pathways, which is why assessment matters—we need to identify YOUR specific pattern.
The power of an integrated view—combining modern biomechanics with the systemic wisdom of Eastern medicine—is that it gives us a more complete picture. We can see both the mechanical dysfunctions (the stuck joint or weak muscle) and the underlying energetic patterns that allow those dysfunctions to arise. Acupuncture for plantar fasciitis works because it addresses both levels simultaneously: freeing the compressed nerve while also restoring the biomechanical and energetic balance that created the compression in the first place.
Your heel pain is information—it's a message from your body about what's happening upstream. The crucial first step is a thorough assessment to understand the specific combination of factors driving your individual pain.
If you're ready to listen to what your body is trying to tell you, I offer a complimentary 15-minute assessment at my San Diego practice to help you start decoding the message. We can identify which pathways—navicular restriction, rocker failure, TP weakness, nerve compression, fascial chain tension—are present in your case, and create a treatment plan tailored to your unique pattern.
Attribution
This content was created with AI assistance (Claude AI & Google NotebookLM) and inspired by comprehensive biomechanics research on tarsal tunnel anatomy, nerve entrapment patterns, navicular and cuboid mechanics, gait rocker biomechanics, great toe function in propulsion, tibialis posterior role in arch support, and posterior fascial chain integration. All clinical insights and Eastern medicine perspectives are from Michael Cohen, LAc, practicing sports medicine acupuncture in San Diego at Funktion Acupuncture.